
Runners Knee / ITBS
ITBS (liotibial Band Syndrome) is the most common cause of pain on the outer side of the knee. Primarily occurring in runners, it is also known as runner’s knee.
It is caused by the tractus rubbing on the femoral condyle, which leads to irritation and pain.
Triggers can be both systemic or muscular, and can be treated using insoles, proper running shoes, regular stretching, and physical therapy.
Cryotherapy, taking a break from running, and topical ointments may help when pain is acute.
ATTENTION: Sensations of pain are often projected towards the top of the tibia, meaning that the cause is often misdiagnosed. It is therefore advisable to do an MRI in addition to the clinical examination.
More questions?
Our experts are happy to help you
Just give us a call!
This is a pain syndrome that primarily occurs in runners and is therefore also known as runner's knee . Additional synonyms include: iliotibial band syndrome (ITBS) or band syndrome, as it affects the iliotibial band. The iliotibial band is a strip of fascia (fascia is a wide, stretching, tendon-like sleeve that covers the muscles) that supports the musculature on the lateral side of the thigh and runs from the iliac crest downwards to anchor at the head of the tibia.

Pain therefore primarily occurs when the band rubs on the protrusion of the femur joint (epicondyle), like a rope on the edge of a cliff. This can lead to overexertion and irritation of the skin on the leg and bursa, mainly in long-distance runners or mountain climbers. ITBS occurs particularly frequently after longer periods of running down mountains - it is a syndrome, however, that is known to be painful for many long distance runners.
ITBS is generally the most frequent cause of pain on the lateral side of the knee. It is also widespread in cyclists.
ITBS often occurs in runners who have the following problems:
- varus leg axes (bowlegs)
- overpronation when pushing off
- weakness of the pelvic stabilizers, with the non-weight-bearing hip sinking and thus pulling excessively on the band.
SYMPTOMS
ITBS is indicated as harmless, however, the pain can be markedly severe and stabbing, making running impossible (I myself had ITBS when taking part in the Florence marathon). The fact that the pain only occurs when starting to run is typical for band syndrome, but it can also be noticed when walking. Some runners are taken away from training for months as a result of band syndrome and inadequate treatment.
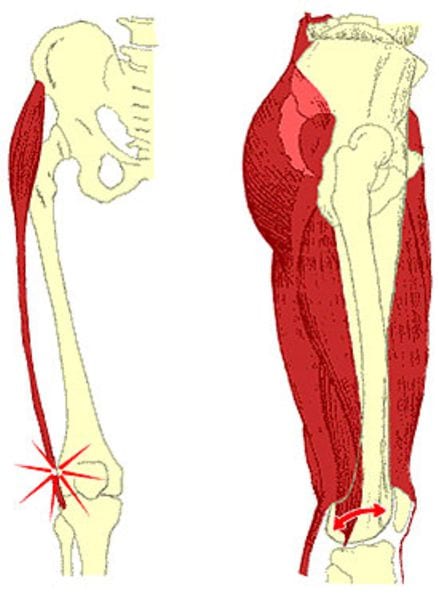
Where the iliotibial band runs to the head of the tibia, the pain that comes from the epicondyles (see above) projects into the knee joint or the lateral side of the tibia head. The projection of pain towards the head of the tibia is often a reason for misidentification of the cause. As a result, many runners have been treated unsuccessfully treated for meniscus and cartilage problems, despite the actual problem being ITBS.
DIAGNOSIS
There is typically a creaking above the femoral condyles, sometimes also a sort of crackling, indicative of irritated tissue. The area is often tender when palpitated. In there is doubt about the diagnosis, it is advisable to get an MRI, which can also rule out other causes.
TREATMENT
In the acute phase, the following steps are imperative: Cryotherapy, a break in training (including cycling as the band rubs over the condyles here too), anti-inflammatory ointments and patches (with Diclofenac or something similar), consistent stretching exercises, strengthening exercises for the pelvic stabilizers and the stomach and back muscles.
Physiotherapy is a must to get the ITBS symptoms under control. Exercises to stretch the often shortened band must be learned and carried out, preferably in combination with active friction therapy by the physiotherapists caring for the patient.
In the case of bowlegs, athletic insoles should be prescribed when necessary. The majority of runners that come to me for surgery with band syndrome, however, are overpronators who have been running with ill-fitting running shoes. Carrying out a treadmill analysis in a specialised shop to make sure you are running with the correct shoes is very crucial .
Once pain has disappeared and you want to slowly begin training again, you must warm up the region of the band around the knee before doing any sport (either with a heater or with thermal ointment). Exercises to stretch the lateral thigh musculature (primarily the tensor fasciae latae muscle) are very important, e.g. crossing the legs when standing or lying down.
Long-distance runs should be avoided in the first few weeks after recommencing training. Cooling with ice packs must be carried out after exercise.
Running downhill should be avoided.
In the event that all these measures prove unsuccessful, or if you are close to a marathon that you have been training for for months, infiltration with cortisone can lead to a rapid improvement in the symptoms.
Once all conservative treatment measures have been fully exhausted without success, an operation can alleviate or lead to significant improvement in the symptoms. The band is cut in a z-shape during this operation and is lengthened and relieved as a result. In runners with very pronounced O-legs, straightening of the legs should certainly be discussed.
More questions?
Our experts are happy to help you
Just give us a call!




