
Medically reviewed by: Univ. Prof. Dr. Christian Gäbler
Last updated: 30.01.2026 | Reading time: approx. 9 min.
The meniscus acts as a shock absorber and provides stability to the knee joint. Due to sports and daily wear and tear, the meniscus’s fibrous cartilage is often subjected to significant pressure and wear. It’s no wonder that a meniscus tear is one of the most common knee injuries.
At the Sportambulatorium Wien, we treat both acute meniscus injuries caused by sport or an awkward movement, and degenerative meniscus tears that may result from decades of wear and tear. Depending on the type of injury, we will find the most suitable treatment for your meniscus tear.

The meniscus & possible injuries
This is how the meniscus is structured
The meniscus consists of fibrocartilage, a rubbery substance similar to that found in the intervertebral discs of the spine. A distinction is made between the medial meniscus and the lateral meniscus. The cartilage is crescent-shaped and acts as a shock absorber between the thigh and lower leg. Furthermore, thanks to its shape, the meniscus supports the knee joint in optimal movement and stabilises the knee together with collateral ligaments and cruciate ligaments.
How does a meniscus tear occur?
If the meniscus is injured and its structure is damaged, this is referred to as a meniscus tear. This injury can occur in two ways:
- Acute meniscus tear: Acute injuries are usually sports injuries, often sustained whilst skiing, playing football, tennis or practising martial arts. However, a meniscus injury can also occur in everyday life as a result of a sudden twisting movement when standing up from a squatting position or other awkward movements.
- Prof. Dr Gäbler says: “In my many years of practice, I have identified two typical causes: an acute tear following an awkward twisting movement under strain (e.g. whilst skiing or playing football) – and degenerative damage caused by chronic overuse. The medial meniscus in particular is significantly more prone to injury due to its firm anchoring in the knee.”
Univ. Prof. Dr. Gäbler sagt: „In meiner langjährigen Praxis sehe ich zwei typische Ursachen: den akuten Riss nach einer ungünstigen Drehbewegung unter Belastung (z.B. beim Schifahren oder Fußballspiel) – und die degenerative Schädigung durch chronische Überlastung. Gerade der Innenmeniskus ist aufgrund seiner festen Verankerung im Knie deutlich verletzungsanfälliger.“
What type of meniscus tear is it?
For us as treating doctors, determining the type, location and nature of a meniscus tear is a crucial step in deciding on the appropriate treatment. In doing so, we look for the following characteristics:
- The direction and location of the crack
- Type of injury: a clean tear (often seen in acute injuries) or a frayed tear (degenerative meniscus tear)
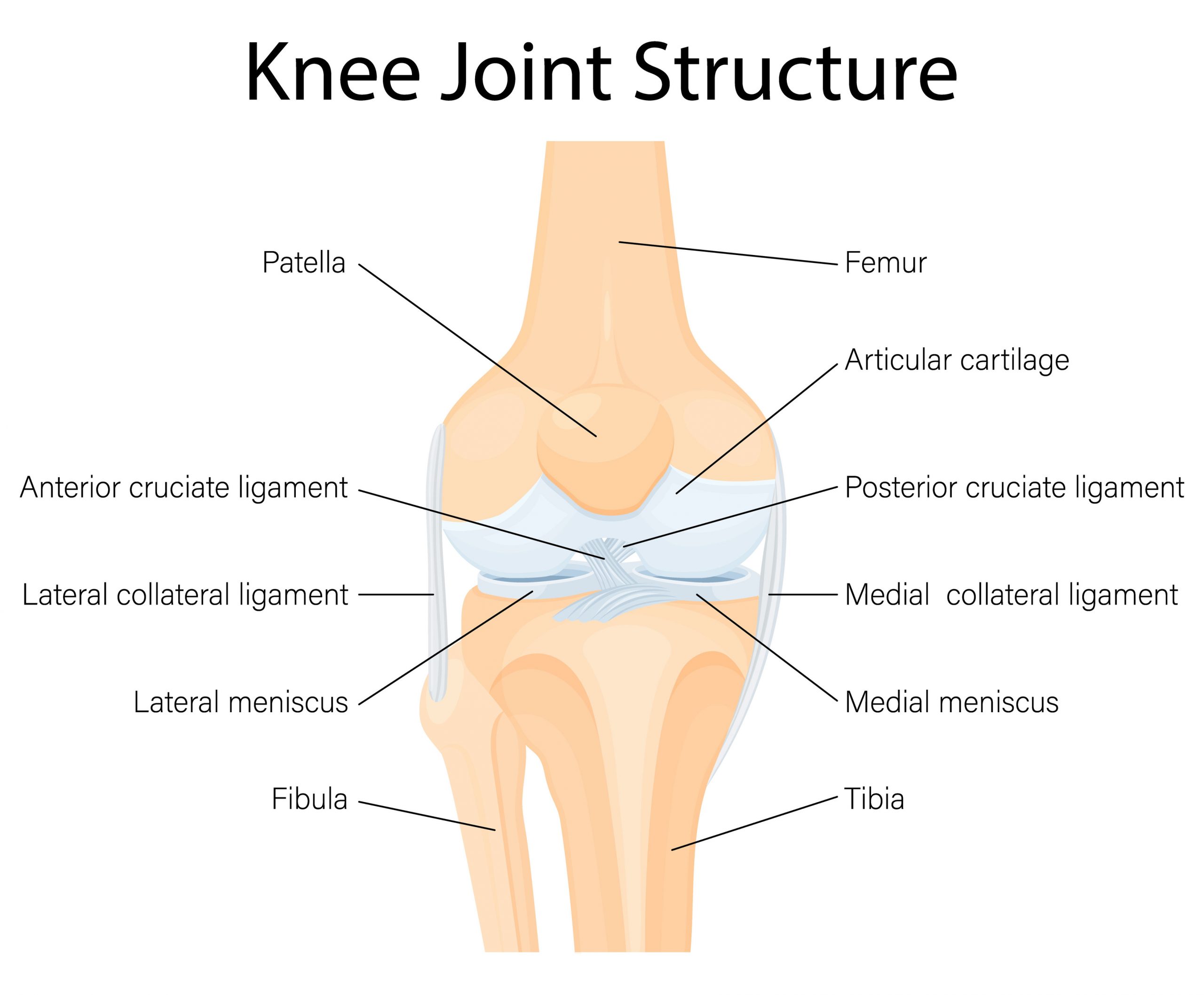
An overview of the different types of meniscus tear:
| Type of meniscus tear | Description and special features |
|---|---|
| Longitudinal crack / Vertical crack | Runs parallel to the direction of the fibres in the meniscus. It frequently occurs in younger people following sports injuries. |
| Tear in the basket handle | A specific type of longitudinal tear in which part of the meniscus folds back into the joint like a handle. This often leads to painful locking. |
| Radial crack / Transverse crack | This tear runs from the inner edge of the meniscus outwards. It severely compromises the stability of the meniscus. |
| torn flap | A tear that is usually oblique, in which a piece of tissue (‘flap’) is free to move and can become trapped in the joint. |
| Horizontal crack | Divides the meniscus into an upper and lower layer. This condition is often caused by degeneration and is more common in older people. |
| Root fracture | A tear directly at the point where the meniscus attaches to the tibial plateau. As the meniscus’s cushioning function is completely lost here, the risk of osteoarthritis is particularly high. |
Why is the location of a meniscus tear important?
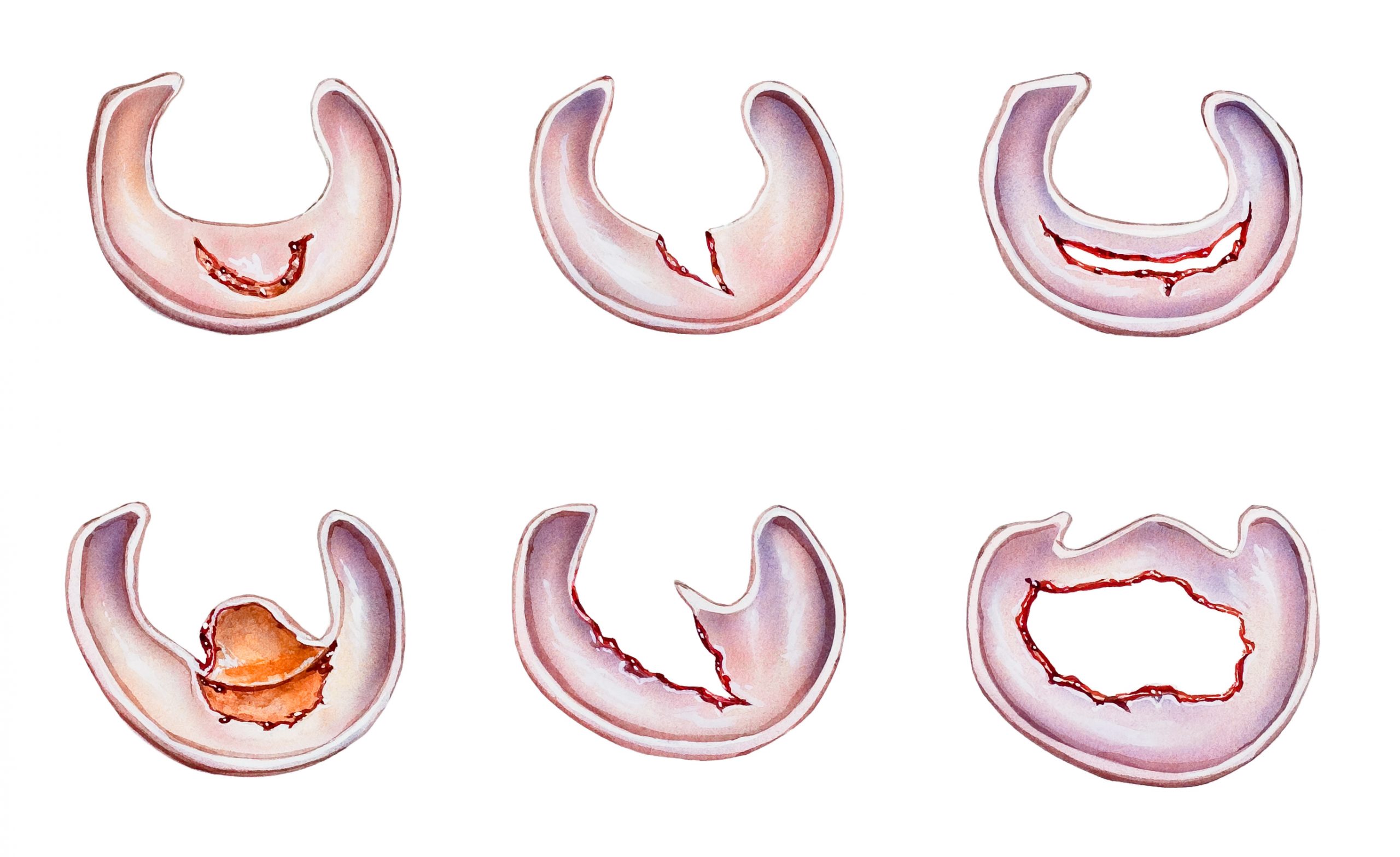
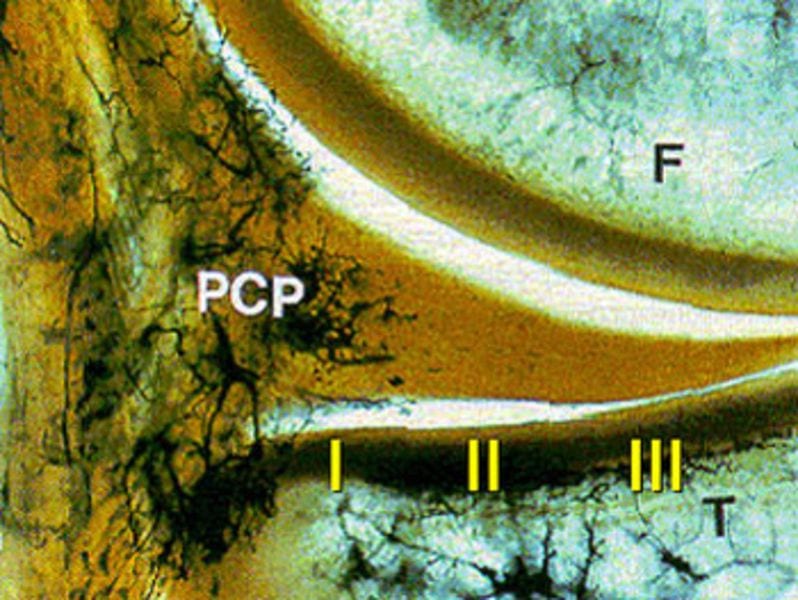
The meniscus is divided into three zones, which indicate the blood supply to the tissue.
- The Zone I or ‘Red Zone’ is located at the edge of the cartilage structure and has the best blood supply. Consequently, the chances of healing are highest here.
- Zone II is located in the centre and already has a reduced blood supply.
- Zone III or the “white zone” is located in the interior, where torn tissue often needs to be removed.
Meniscus tear: symptoms & signs
The specific symptoms depend largely on the type and location of the tear. Common symptoms of a meniscus tear include:
- Shooting pain: A sharp, localised pain directly over the joint space is a common symptom of a meniscus tear. This pain often worsens during twisting movements, when climbing stairs or when squatting deeply.
- Swelling: Following an injury, the knee often responds with an inflammatory reaction and becomes visibly swollen (joint effusion). The knee feels tight and its range of motion is restricted.
- Mechanical blockages: If, following an injury, a piece of the meniscus becomes lodged in the joint, the knee can no longer be fully straightened or bent. This can feel like a “snapping” or “clicking” sensation in the joint and significantly restricts the movement of the knee joint.
- Feeling of instability: The feeling that the knee might ‘give way’ at any moment.
Symptoms of acute and degenerative meniscus tears
The symptoms experienced with a meniscus tear can also vary depending on the type of injury.
Acute or traumatic meniscus tears are often accompanied by sudden pain. After twisting the knee or taking a quick lunge, you feel a sudden twinge and notice swelling.
Degenerative damage, on the other hand, tends to manifest itself as a dull, exertion-related pain that initially subsides after periods of rest but regularly returns when activity resumes.
Do you have sharp pains in your knee joint?
Play it safe. Book your appointment for a clinical examination now.
Just give us a call!
Diagnostic options following a meniscus tear
To diagnose a meniscus tear with certainty, we at the Sportambulatorium Wien always use a multi-stage diagnostic procedure: a clinical examination by our specialists and confirmation via imaging, such as an MRI scan.
1. Examination by our specialists
Every diagnosis begins with a consultation with the doctor (medical history) and a physical examination. During this, the orthopaedic surgeon palpates the joint space and performs specific tests (e.g. the McMurray- or Steinmann test). The leg is bent and rotated at specific angles. Pain or an audible click during these movements already gives us a very reliable indication of which part of the meniscus is affected.
2. Imaging techniques for meniscus tears
2.1. Magnetic resonance imaging (MRI)
An MRI scan provides the most comprehensive diagnosis of a meniscus tear. Unlike an X-ray, an MRI scan provides a detailed view of soft tissues such as cartilage, ligaments and menisci. The cross-sectional images allow the doctor not only to see that a tear is present, but also to determine its exact shape and location. This is crucial when deciding whether surgery is necessary.
2.2. X-ray
A standard X-ray cannot show the meniscus itself. However, X-rays do help to rule out other causes of knee pain. Among other things, they can reveal advanced joint wear (osteoarthritis), which often goes hand in hand with meniscus damage.
2.3. Ultrasound (sonography)
An ultrasound scan is a quick way to get an initial assessment of a meniscus tear. It is particularly useful for the doctor to identify associated symptoms such as joint effusion (fluid build-up) or cysts (e.g. a meniscal ganglion). However, an ultrasound scan is less suitable for diagnosing a meniscus tear itself.
2.4. Arthroscopy (joint examination)
During arthroscopy, the surgeon can view the meniscus directly via a camera and assess its stability. This makes it the most accurate diagnostic method available. However, this minimally invasive procedure is now almost exclusively performed when the diagnosis has already been confirmed by an MRI scan and surgical treatment is carried out at the same time.
Tip: An MRI scan is always recommended, as there are some meniscus injuries that do not require surgery.
Meniscus tears and other knee injuries
A meniscus tear often occurs alongside other problems and injuries in the knee.
Meniscus ganglion
A meniscus ganglion is a cyst that forms at the base of the meniscus and can develop as a result of a meniscus tear. A ganglion is usually filled with a jelly-like fluid and can cause additional pain in the knee. To treat the ganglion successfully, it is essential that the meniscus tear is also treated. We do not recommend removing the ganglion alone without addressing the underlying cause.
Cruciate ligament tear and meniscus tear
A cruciate ligament tear and a meniscus tear often occur together. The cruciate ligaments stabilise the knee, and therefore a cruciate ligament tear often leads to abnormal mobility of the joint. This instability places a massive strain on the menisci and frequently causes secondary tears. With this combined injury, surgery is usually unavoidable in order to restore stability to the joint and prevent long-term damage.
Collateral ligaments and meniscus injuries
The collateral ligaments, particularly the medial collateral ligament, are anatomically fused with the meniscus. In accidents involving lateral force or severe twisting, the collateral ligaments and meniscus are therefore often injured at the same time. In treatment, stabilising the ligaments is often the top priority, so that the meniscus is also protected from long-term damage.
Good to know: When the cruciate ligament, collateral ligaments and meniscus are all affected by an injury, this is referred to in medicine as the “unhappy triad”. It is often caused by a severe sports injury or an accident and requires surgery and intensive rehabilitation.
Treatment: Does a meniscus tear always require surgery?
When meniscus damage is diagnosed, surgery is very often recommended – even if there is little or no pain. However, there are also cases where a meniscus tear does not require surgery. The actual decision regarding the form of treatment must, however, be made on an individual basis for each patient.
Why is surgery usually the best option for a meniscus tear?
As the meniscus has very little blood supply and is unable to heal on its own, preventive surgery is often the best treatment method. This is because the damaged meniscus causes rapid damage to the cartilage and joint through constant friction against the cartilage.
Prof. Gäbler recommends: “The basic rule is: the younger a patient with a meniscus tear is, the sooner they need to have surgery. The older patients with degenerative tears are, the more likely it is that we will try to relieve their pain without surgery.”
Meniscus tear without surgery
A tear can be treated conservatively (physiotherapy and muscle strengthening) if:
- … there are no blockages or persistent pain.
- … targeted muscle strengthening can effectively relieve pressure on the knee and the cartilage.
- … there is a chance of self-healing due to the location of the tear (in Zone I).
- … surgery poses an increased risk to the patient’s general health.
- … existing osteoarthritis is already so advanced that meniscus surgery alone will not alleviate pain or achieve the desired therapeutic goal.
Can a meniscus tear heal on its own?
The short answer is: Yes, self-healing is possible, but in most cases unlikely. A good chance of healing exists only in Zone I, as blood supply – and thus the tendency to heal – decreases steadily inwards towards Zone III. The duration of healing for a meniscus tear without surgery cannot be answered in general terms, but is typically several weeks.
When is meniscus tear surgery necessary?
There are clear medical indications that make surgical intervention (arthroscopy) absolutely necessary. This is particularly the case when the mechanical function of the joint is immediately impaired or long-term damage needs to be prevented.
| Criterium | Reason for the surgery |
|---|---|
| Mechanical blockages | If the knee ‘locks up’ and can no longer be straightened, surgery is usually necessary. |
| Unstable crack patterns | Large lacerations or radial tears can tear further under stress and damage healthy tissue. |
| Erfolglose konservative Therapie | If, despite intensive physiotherapy over a prolonged period, there is no improvement in pain or physical capacity. |
| Young, active patients | People who are physically active often undergo surgery at an early stage in order to restore full functionality in the long term. |
| Multiple injuries | If the tear occurs alongside a cruciate ligament tear or damage to the collateral ligaments, surgery is usually required to ensure the overall stability of the knee. |
| Repairable cracks | If the tear is located in a well-perfused area and can be sutured (meniscal repair), this should be done as soon as possible in order to save the meniscus. |
The risk of osteoarthritis following a meniscus tear without surgery
The pain caused by a meniscus injury rarely subsides on its own, as the meniscus has a poor blood supply and is unlikely to heal naturally. The constant friction caused by the damaged meniscus in untreated meniscus injuries leads to recurring pain on weight-bearing, locking of the joint, swelling of the knee joint and secondary damage to the cartilage surfaces, resulting in premature osteoarthritis.
Meniscus tear surgery: methods in detail
If surgery is necessary, a minimally invasive arthroscopy is performed. At the Sportambulatorium Wien, our primary aim is always to preserve as much meniscus tissue as possible. There are two main procedures used in meniscus surgery:
Meniscus repair (meniscus suturing)
In meniscal repair, the torn meniscus is not removed but is surgically repaired and sutured. For the suture to heal successfully, the tear must be located in the well-vascularised ‘red zone’.
The refixation procedure:
- During arthroscopy, the surgeon inserts a camera and special instruments into the joint to precisely realign the edges of the tear.
- These are then permanently secured using very fine sutures.
- The aim of this procedure is to preserve the meniscus’s natural shock-absorbing function.
- Partial meniscus removal (partial resection) & smoothing
Meniskus Teilentfernung (Teilresektion) & Glättung
In a partial removal or partial resection, the cartilage tissue is trimmed and then smoothed during arthroscopy. In this procedure, the surgeon does not remove the entire meniscus, but only the torn, unstable part that is causing the symptoms.
Procedure for the resection:
- During the arthroscopy, a camera and special micro-instruments are inserted into the knee.
- The surgeon removes only the damaged tissue that is blocking the joint or causing pain.
- The remaining edges of the meniscus are carefully smoothed to prevent new tears from forming and to ensure the meniscus sits securely in the joint again.
- Aim of the procedure: to remove dead tissue and restore full mobility to the knee joint
Good to know: The more meniscus tissue that needs to be removed, the more likely it is that premature joint wear (osteoarthritis) will occur. Targeted physiotherapy and mindful movement can help prevent this wear and tear.
Partial resection vs. meniscal repair
| Characteristic | Meniscus suture (refixation) | Partial meniscus resection |
|---|---|---|
| Procedure | The tear is sutured using special sutures. | The damaged tissue is removed and the remaining tissue smoothed out. |
| Objective | Complete preservation of the meniscus as a shock absorber. | Rapid relief from pain and elimination of joint locking. |
| Prerequisite | Tear in the well-vascularised ‘red zone’ | Usually for degenerative tears or in the ‘white zone’ |
| Healing time | Protracted (approx. 4–6 months before returning to sport). | Quick (approx. 4–6 weeks before returning to sport). |
| Aftercare | Often 6 weeks in a splint (orthosis required) and partial weight-bearing. | Full weight-bearing usually possible after a few days. |
| Long-term consequences | Low risk of osteoarthritis, as the cushioning function is retained. Risk of re-tearing | Increased risk of osteoarthritis, as less cushioning surface remains. |

Recovery time & rehabilitation following a meniscus tear
Restrictions on sporting activities following surgery
The time taken for full recovery and a return to sport varies depending on the type of treatment or surgical method used. In our experience, no sporting restrictions are to be expected following meniscus surgery. However, the return to various sports depends on the surgical method and the extent of the damage to the meniscus tissue.
Recovery timeline without surgery
A meniscus tear treated without surgery usually takes 3 to 6 months to return to full weight-bearing capacity and sporting activities.
- Weeks 1–2: The focus is on pain relief and reducing swelling. Weight-bearing is generally limited to what is pain-tolerable (possibly with crutches).
- Weeks 2–6: Targeted strengthening of the thigh muscles (physiotherapy) to relieve pressure on the joint. Mobility is gradually increased. Gentle exercise without much resistance, e.g. on an ergometer, is appropriate provided there is no pain.
- Weeks 6–8: Joint-friendly sports such as cycling, walking or front crawl swimming are permitted.
- From month 3: The meniscus continues to stabilise, and the muscles increasingly take over the protective function. Light running training or jogging on soft ground is possible.
- From 6 months: If the training so far has progressed well, stop-and-go sports such as football, tennis, basketball and even skiing are now possible again.
Recovery schedule following a partial meniscectomy
Following a partial removal of the damaged meniscus, weight-bearing on the leg is possible immediately, provided the patient’s pain levels allow it. Crutches, if used at all, are only required for a few days.
- Week 1: Weight-bearing on the joint, walking and strolling, is possible immediately.
- Weeks 2–3: Cycling (exercise bike), light swimming (front crawl).
- Weeks 4–6: Jogging on flat ground, light strength training.
- Weeks 6–8: Provided the knee is no longer swollen and movement is possible without pain, stop-and-go sports (football, tennis) can also be resumed.
Recovery timeline following refixation
Recovery following meniscus suturing is a lengthy process, and patients must not put any weight on the operated leg for up to six weeks.
- Weeks 1–6: Rest is now essential. Movement with crutches and partial weight-bearing is possible. A splint limiting flexion to 60° or 90° can help to relieve pressure on the suture.
- Weeks 7–12: The transition to full weight-bearing is possible. Mobility can be improved by cycling on an exercise bike.
- Months 3–4: If healing is successful, light walking and jogging can now be started.
- Months 6–9: Sports involving twisting movements (football, skiing, basketball) are only safe again after at least 6 months.
Special cases: Meniscus tears in children and the elderly
At the Sportambulatorium Wien, we ensure that everyone receives personalised treatment. This means that both the youngest and the oldest patients receive the appropriate therapy
Meniscus tears in children & adolescents
Meniscus tears in children are almost always the result of acute sports injuries or anatomical variations. Furthermore, a meniscus injury in children and adolescents can differ significantly from injuries in adults.
- The discoid meniscus: A distinctive feature in children is the congenital discoid meniscus. In this condition, the meniscus is not crescent-shaped but forms a full disc. This shape is less stable and is prone to tears or painful ‘snapping’ in the knee even under minimal strain.
- Higher potential for healing: As the tissue in children is still significantly better supplied with blood (the ‘red zone’ is wider than in adults), the chances of spontaneous healing or a successful meniscus suture are higher.
- Preservation is the top priority: As children still have many decades of joint stress ahead of them, we almost always attempt to suture the meniscus in children.
Are you concerned about your child's knee injury?
Go here for the specialist consultation for children and teenagers
Go here for the specialist consultation for children and teenagers
Meniscus tears in older adults (over 60)
In patients over the age of 60, a meniscus tear is often the result of wear and tear. This is because, as we age, cartilage loses its elasticity and becomes more brittle. Often, a simple, awkward everyday movement – such as a slight twist when getting out of a car – is enough to cause a tear in a meniscus that is already damaged.
We pay particular attention to the following points in older patients:
- Link to osteoarthritis: Often, when meniscus problems arise in older age, it is not just the cartilage tissue that is affected, but also the onset of joint wear and tear. Pain management and treatment are therefore tailored specifically to this.
- Conservative treatment before surgery: In older patients, the benefits and risks of meniscus surgery are weighed up more carefully. This is because surgery is not always the best option, particularly in cases of severe wear and tear, and physiotherapy is usually a good course of treatment.
- Everyday mobility is the primary goal: Often, the aim of successful treatment in older patients is not necessarily a return to sport, but rather pain reduction and everyday mobility
Conclusion: A common injury with a good prognosis
A meniscus tear can occur following a sports injury or as a result of years of wear and tear, and in both cases it is an injury that responds well to treatment. In most cases, arthroscopic surgery is required to restore full range of motion and reduce pain. However, conservative treatment involving physiotherapy and muscle strengthening is also an option.
Are you experiencing pain or knee instability? At Sportambulatorium Wien, we will find the right treatment for you following a comprehensive diagnosis!
Vereinbaren Sie jetzt Ihren Termine:
💬 Online via Kontaktformular
📞 Tel: 01 4021000
✉️ Mail: office@sportambulatorium.wien
You may also be interested in



Scientific sources & studies
The content of this page is based on the clinical experience of Univ. Prof. Dr. Gäbler and current international studies in sports traumatology:
- Vergleich: OP vs. Physiotherapie bei jungen Patienten: van der Graaff SJA et al.: Arthroscopic Partial Meniscectomy Versus Physical Therapy for Traumatic Meniscal Tears in a Young Study Population. Erschienen in: British Journal of Sports Medicine. 2022.
- Langzeitfolgen (MRT) nach Operation oder Training: Clausen SH et al.: Two-Year MRI-defined Structural Damage and Patient-Reported Outcomes Following Surgery or Exercise for Meniscal Tears in Young Adults. Erschienen in: British Journal of Sports Medicine. 2023.
- Therapie degenerativer Meniskusrisse: Hohmann E: Treatment of Degenerative Meniscus Tears. Erschienen in: Arthroscopy: The Journal of Arthroscopic & Related Surgery. 2023.
- Strategien zum Meniskuserhalt (Save the Meniscus): Beaufils P, Pujol N: Management of Traumatic Meniscal Tear and Degenerative Meniscal Lesions. Erschienen in: Orthopaedics & Traumatology, Surgery & Research (OTSR). 2017.




